Pathology of the Integumentary System
Integumentary System Conditions
- Skin cancer
- Carcinoma: cancer of the epithelial tissue
- Acne: images
- Cause: hormone-related changes in sebaceous glands on the face, neck, chest, back, shoulders, combined with bacterial infection in inflammatory acne. Affects more than 85% of teenagers; can continue into adulthood.
- Signs and Symptoms: noninflammatory blackheads; inflammatory pustules (whiteheads). Severe acne can lead to scarring and/or psychological distress.
- Indications: No systemic reasons for people with acne to avoid massage.
- Contraindications: Avoid lesions.
- Impetigo: images
- Cause: bacterial skin infection
- Signs and Symptoms: rash, sometimes with blisters and/or crusts
- Indications: None
- Contraindications: Absolute; highly contagious. Do not massage until lesions have completely healed.
- Cellulitis: images
- Cause: bacterial skin infection that can go systemic
- Signs and Symptoms: redness, tenderness, fever, headache, malaise, systemic infection
- Indications: None.
- Contraindications: Absolute; do not massage until infection is completely cleared up.
- Herpes simplex: images
- Cause: Herpes simplex virus
- Signs and Symptoms: Lesions: cold sores or fever blisters on face/mouth or genital region, tingling, itching, pain, blisters, secondary infection, psychological distress, social isolation
- Indications: Yes, unless there is any systemic infection (but use strict infection control precautions, such as washing hands, cleaning and bleaching surfaces and sheets)
- Contraindications: Lesions contagious; do not touch; do not touch objects that have come into contact with lesions.
- Chickenpox: images
- Cause: Varicella zoster virus, spread by (probably) respiratory route
- Signs and Symptoms: skin rash and blisters (dew drop) that breaks and crusts over, itching, respiratory symptoms
- Indications: Wait until client is fully recovered before massaging.
- Contraindications: Do not massage.
- Shingles (Herpes zoster): images
- Cause: Varicella zoster virus
- Signs and Symptoms: painful (often described as stinging, tingling, or throbbing) skin rash with blisters in a limited area on one side of the body along infected dermatomes.
- Indications: None--most people with shingles are in too much pain to tolerate massage well.
- Contraindications: Wait until lesions have healed and are no longer painful
- Wart (Verruca vulgaris): images
- Cause: Human papillomavirus (HPV) types 1, 2, and 3 (not the same HPV types as anogenital warts or cervical cancer).
- Signs and Symptoms: small rough tumor resembling a cauliflower or blister. They typically disappear after a few months, but can last for years and can recur.
- Indications: Ok to massage elsewhere than warts themselves.
- Contraindications: Local; practice strict infection control. Warts are contagious from skin of infected person, or from towels or other objects they have handled.
- Ringworm: images
- Cause: Tinea: a general term for conditions where fungi overcome the body's resistance and establish an infection. Tinea capitis: scalp ringworm images; Tinea cruris: jock itch, "crotch rot" images; Tinea pedis: Athlete's foot images
- Symptoms: reddened circular itchy patches that can be spread by scratching. Athlete's foot can cause peeling of skin.
- Indications: Ok to massage unless systemic infection is present.
- Contraindications: Do not touch lesions; practice strict infection control, as lesions can be spread by scratching or by touching objects harboring the fungus.
- Scabies: images
- Cause: parasitic mite
- Signs and symptoms: itching, burrowing, secondary infection, rash, secondary infection.
- Indications: none. Probably best to avoid massage because of major infection risk.
- Contraindications: Avoid infected area. Practice strict infection control.
- Psoriasis: images
- Cause: autoimmune. Possibly a genetic component.
- Signs and Symptoms: affects the skin and joints, often elbows and knees. It commonly causes pink or red scaly patches to appear on the skin. Can have a huge impact on quality of life.
- Indications: Massage ok in subacute stages.
- Contraindications: Avoid lesions during acute stages.
- Scleroderma: images
- Cause: chronic autoimmune disorder
- Signs and Symptoms: hardening or sclerosis in the skin or other organs
- Indications: Massage as tolerated by patient, unless advanced circulatory or kidney damage is present. Scleroderma philanthropic organizations recommend massage for symptom relief and improved quality of life.
- Contraindications: Depends on patient; massage may be adapted to be less vigorous for more frail clients.
- Eczema: images
- Cause: The term eczema refers to a set of clinical characteristics. Eczema is a form of dermatitis, or inflammation of the epidermis. Classification of the underlying diseases has been haphazard and unsystematic, with many synonyms used to describe the same condition. Some cases of eczema can be caused by allergy.
- Signs and Symptoms: dryness and recurring skin rashes which are characterized by one or more of these symptoms: redness, skin edema (swelling), itching and dryness, crusting, flaking, blistering, cracking, oozing, or bleeding.
- Indications: Massage ok, depending on patient, as long as systemic inflammation is not present.
- Contraindications: Local.
- Decubitus ulcer, pressure sores, bedsores: images
- Cause: Pressure, especially of bony extremities, against surfaces, due to immobility, prolonged bed rest, paralysis, or other conditions that restrict motion.
- Signs and Symptoms: See descriptions/illustrations of Stages I-IV.
- Indications: Controversial. Some authorities say light massage is helpful for Stage I; all agree not to massage in later stages. There is a responsibility to report cases of neglect, and bedsores are a sentinel event (an event that triggers an alarm) of poor nursing care.
- Contraindications: Do not massage.
- Traumatic Burns
| Basal cell carcinoma | Squamous cell carcinoma | Melanoma | |
| Cell Type | epithelial cells in basal layer | squamous epithelial cells (keratinocytes) | melanocytes |
| Metastasis/Mortality rate | Lowest of these 3 types | Next lowest of these 3 types | Highest of these 3 types |
| How common? | Most common of these 3 types. The most common of all types of skin cancer; approximately 800,000 new cases yearly in US. Approximately 3 out of 10 Caucasians develop a basal cell cancer within their lifetime. Sunscreen protects. | Next most common of these 3 types. Incidence of squamous cell carcinoma (SCC) varies with age, gender, race, geography, and genetics. The incidence of SCC increases with age and the peak incidence is usually around 66 years old. Males are affected with SCC at a ratio of 2:1 in comparison to females. Caucasians are more likely to be affected. Sunscreen protects. | Least common of these 3 types. Sunscreen may not protect; this is currently being researched. |
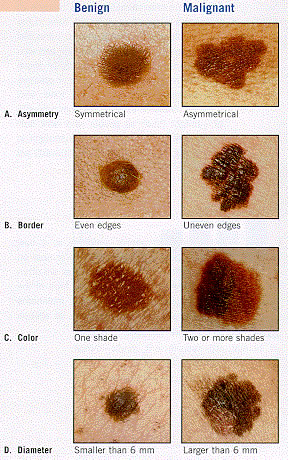
| Signs and symptoms | sore that does not heal, may be painless, may bleed, may itch | sore that does not heal, may be painless, may bleed, may itch | mole that exhibits ABCDs of melanoma: Asymmetrical skin lesion / Border of the lesion is irregular / Color: melanomas usually have multiple colors / Diameter: moles greater than 6 mm are more likely to be melanomas than smaller moles. |
Bacterial Conditions
Viral Conditions
Fungal Conditions
(notice that, despite the name, this is a fungus, not a true worm)
Parasitic Conditions
Miscellaneous Conditions
It is generally accepted that a burn affecting more than one percent of the body surface, (approximately area of the casualty's palm) should be assessed by a medical practitioner.
| First-degree burns | Second-degree burns | Third-degree burns | |
| Involved layers of skin | Epidermis only | Superficial (papillary) dermis; may also involve the deep (reticular) dermis layer. | Epidermis is lost; damage to the subcutaneous tissue. |
| Causes | Heat, cold, electricity, chemicals, light, radiation, friction. Most sunburns can be included as first degree burns. | Heat, cold, electricity, chemicals, light, radiation, friction. | Heat, cold, electricity, chemicals, light, radiation, friction. |
| Signs and symptoms | Redness (erythema), a white plaque and minor pain at the site of injury. | Erythema with superficial blistering of the skin; can involve more or less pain depending on the level of nerve involvement. | Charring and extreme damage of the epidermis; sometimes hard eschar will be present. Scarring and loss of hair shafts and keratin. These burns may require grafting. Scarring and deformity may cause psychological distress. |
| Healing time | 3-6 days | Depends on severity of burn | Depends on severity of burn |
| Massage indicated? | Acute phase: No Subacute phase: Local contraindication, and to pain tolerance of client Chronic phase: Local contraindication, and to pain tolerance of client | Acute phase: No Subacute phase: Local contraindication, and to pain tolerance of client Chronic phase: Local contraindication, and to pain tolerance of client | Acute phase: No Subacute phase: Local contraindication, and to pain tolerance of client Chronic phase: Local contraindication, and to pain tolerance of client; possible treatment of scar tissue |

{kind=link}
{kind=link}